
Management of UO, Addisonian Crisis, and Anaphylaxis Cases for General Practice and Urgent Care Veterinarians
Insights from our recent webinar by DVM STAT Criticalist & Founder, Kristin Welch, DVM, DACVECC.
In DVM STAT’s recent CE webinar on Urgent & Emergent Cases in General Practice, Kristin Welch, DVM, DACVECC shared practical, evidence-based guidance on recognizing, stabilizing, and optimizing outcome in feline urethral obstruction, hypoadrenocorticism cases and canine anaphylaxis cases.
Missed the live CE?
You can still take the free course on-demand and receive 1 hour of RACE-approved CE here and check out our entire live and on-demand CE library here.
Emergent cases have a way of arriving in general practice at the least convenient moment. The blocked cat presents mid-appointment block. The collapsed young dog is carried through the door thirty minutes before close. The vomiting standard poodle is a routine recheck until the bloodwork returns.
What these cases share is that rapid pattern-recognition allows you to promptly stabilize these cases improving patient outcome. The decisions made in the first hour usually determine how the next twenty-four hours unfold. The three cases below are commonly seen in general practice and owners often don’t recognize how critically ill their pet is until your first discussion in-hospital.
“Even if you plan to refer these cases elsewhere, initial diagnosis and stabilization are priorities no matter what type of practice you are in. ”
Feline Urethral Obstruction: Stabilize Then Unblock

The blocked cat is a familiar presentation for all vet teams. A working minimum database includes electrolytes, BUN, creatinine, and an ECG, which is recommended in every UO case regardless of how stable the patient appears. POCUS confirms the distended bladder and rules out preexisting peritoneal effusion. A proBNP is worth running because significant cardiomyopathy meaningfully changes anesthetic protocols and client communication on anesthetic risks.
The clinical question that decides the stabilization priorities is simple: is the potassium above 7.5 mmol/L, and is the patient bradycardic or having arrhythmias? If yes, stabilize first. Bradycardia below 140 bpm combined with hypothermia below 95.9°F carries a positive predictive value greater than 98% for potassium above 8 mmol/L, so the physical exam alone can drive the decision when point-of-care electrolytes are pending.
Fluid therapy remains the fastest path to normokalemia and should not be delayed while waiting to unblock. A 5 to 10 mL/kg bolus of balanced isotonic crystalloid, repeated as perfusion parameters dictate, corrects hypovolemia and decreases (dilutes) potassium while other treatments are instituted. Calcium gluconate counteracts hyperkalemia's effects on cardiac myocyte membrane potential, restoring the gap between resting and threshold potentials for 30 to 60 minutes without lowering potassium, which buys time when arrhythmias are present. Insulin plus dextrose shifts potassium intracellularly and should be paired with blood glucose monitoring every four hours. Terbutaline and/or albuterol can be utilized to drive potassium intracellularly as well. Importantly a recent 2025 JAVMA study shows that there is no therapy that is more effective at lowering potassium levels beyond fluids, calcium gluconate and prompt unblocking. A 2021 JAVMA randomized study of 80 cats confirmed what many clinicians suspected: cystocentesis does not make subsequent catheterization faster or easier. Decompressive cystocentesis remains a useful tool in peri-arrest cats and recent retrospective data support a low complication rate.
Analgesia is a priority and pure mu-agonists are preferred. For anesthesia, a combination of methadone or buprenorphine plus midazolam plus propofol or alfaxalone is the standard. In the critical cat with potassium above 9 to 10 mmol/L, opioid plus benzodiazepine alone may be sufficient to unblock. Ketamine plus diazepam is appropriate when hypertrophic cardiomyopathy is not a concern.
Monitoring in the post-obstructive period is critically important and this is where referral may be indicated for 24-hour care. Post-obstructive diuresis develops in 40 to 67% of cats, and re-obstruction within 24 to 72 hours occurs in 15 to 30%. A 2022 JAVMA study found that prazosin increased the probability of recurrent UO by day 14 (24% with prazosin versus 13% without), a finding that has changed prescribing practices. Most recently, a 2026 JAVMA double blind placebo controlled study showed that lorazepam administered in the 30 days post obstruction resulted in a statistically significant reduction in the recurrence of urethral obstruction in cats.
Canine Hypoadrenocorticism: The Great Pretender

Addison's disease earns its "great pretender" reputation because it presents as vague, chronic, and easily attributed to something else. The clinical clues that should raise suspicion are frequently under-weighted in the initial workup: absence of a stress leukogram in a genuinely sick dog, inappropriate or relative bradycardia in a hypovolemic patient, normal or low-normal blood glucose, and a history of chronic intermittent vomiting, diarrhea, or pelvic limb weakness. Any one of these findings in an emergency case and certainly in a collapsed or hypotensive dog warrants a baseline cortisol before the workup goes further.
The Na/K ratio is more reliable than either value in isolation. A working rule of thumb is sodium below 135 mmol/L and potassium above 5.5 mmol/L, with most confirmed cases showing a ratio below 22. Approximately 10% of hypoadrenocorticism cases present with normal electrolytes (atypical or eunatremic eukalemic), which is why the ratio alone cannot rule the diagnosis out. Azotemia is present in 90% of cases (BUN) and 65% (creatinine). Hypercalcemia appears in about 30% of cases, hypoglycemia in 15%, and anemia in 30%, with the anemia rate climbing to 70% after IV fluid resuscitation unmasks the true degree of GI blood loss.
A baseline cortisol above 2 mcg/dL effectively rules out hypoadrenocorticism, with a sensitivity of 99.4%. This is the screening test that belongs in every workup where the diagnosis is on the differential. Definitive diagnosis still requires an ACTH stimulation test with pre and 60-minute post cosyntropin samples. A practical cost-savings approach is to divide a 250 mcg cortrosyn vial into 1 cc syringes (0.1 or 0.25 mL aliquots) and freeze them in plastic syringes for up to 6 months. Dexamethasone SP does not interfere with ACTH stim results within 24 hours, so treatment does not need to wait for the stim.
Stabilization uses isotonic crystalloids (LRS, Plasmalyte, or Normosol-R) rather than 0.9% saline, with 10 to 20 mL/kg boluses over 20 to 30 minutes and reassessment of perfusion parameters between boluses. For chronic hyponatremia, sodium correction should not exceed 0.5 mmol/hr to avoid central pontine myelinolysis. Dexamethasone SP at 0.2 mg/kg IV, GI protection with a PPI plus or minus sucralfate, and electrolyte rechecks every 4 hours during resuscitation (then every 8 hours) round out the initial stabilization plan. Once DOCP is administered, electrolytes typically normalize within 12 hours.
The discharge plan matters for long-term outcomes. Prednisone starts at a supraphysiologic dose with a 10-to-14-day recheck to taper to a physiologic dose if GI signs have resolved. Electrolytes are rechecked at day 14 and again at day 25 to 28, and the next DOCP dose is administered at 25 to 28 days. Owner education around the "stress steroid dose" is critical: doubling the prednisone dose for 3 days before, during, and 3 days after any stressful event (boarding, travel, surgery, illness) prevents most avoidable crises.
Canine Anaphylaxis: The GI Tract is the Canine Shock Organ
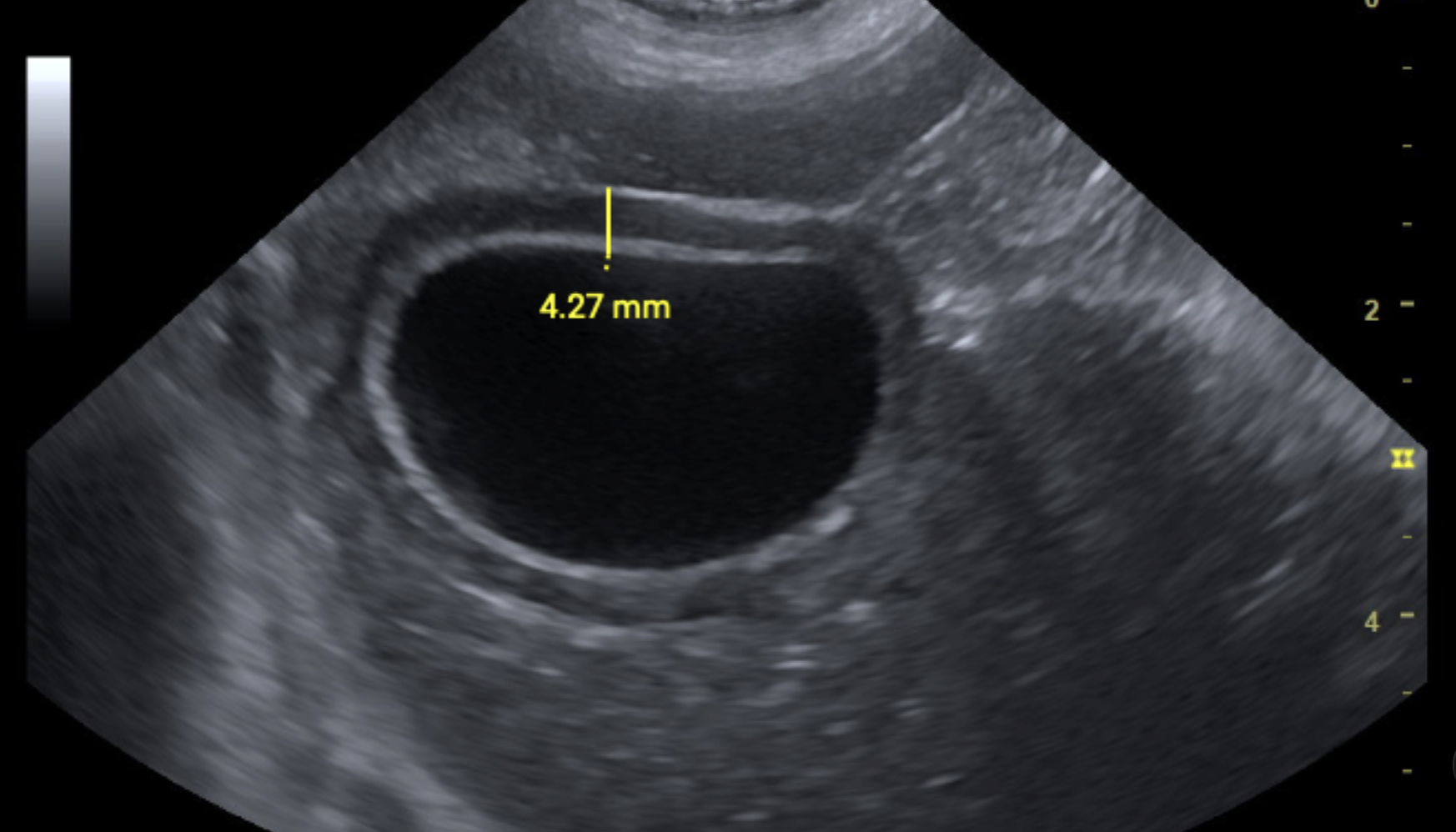
Gallbladder “halo” sign
Most anaphylactic dogs present with vomiting and diarrhea rather than cutaneous signs. Collapse is the third most common presenting complaint. Tachycardia with or without hypotension is typical, and a mild-to-moderate ALT elevation of 300 to 400 U/L appears within hours of the reaction.
The gallbladder halo sign is the single most useful POCUS finding in these cases. A double-walled gallbladder greater than 3 mm thick is 93% sensitive and 97% specific for anaphylaxis, appears in 75 to 98% of canine anaphylaxis cases, and is present in essentially 100% of anaphylactic hemoperitoneum cases. The halo can develop within 2 hours of the reaction, so a normal initial POCUS does not rule anaphylaxis out. A repeat scan at 2 to 4 hours is worth doing when clinical suspicion remains high. Other causes of gallbladder wall edema (pericardial effusion, right-sided heart failure, DCM, cholecystitis) should be ruled out before the finding is attributed to anaphylaxis.
Epinephrine is the first-line treatment, and the historical reflex to reach for diphenhydramine and dexamethasone should be revised. Diphenhydramine does not mitigate the anaphylactic reaction itself; it may relieve urticaria and pruritus but does nothing for the cardiovascular collapse. Glucocorticoids do not improve outcome or survival as a first-line agent, though they have a role in downregulating the late-phase eosinophilic inflammatory response and may reduce biphasic symptoms. A practical epinephrine protocol is reviewed in the webinar.
Anaphylactic hemoperitoneum is a medical, not surgical, presentation. Survival exceeds 90% in retrospective studies with appropriate medical management. About half of these cases have normal PT/PTT and platelet counts, and FFP is reserved for patients with prolonged coagulation times and clinical evidence of bleeding. Hospitalization is typically 2 to 3 days for moderate-to-severe cases, longer than the 24 hours often expected.
Focusing on Hemodynamic Stabilization Saves Lives
Focus on hemodynamic stabilization and avoid diagnostic tunnel vision. The diagnosis becomes clearer the moment the clinician zooms out and addresses the most immediately life-threatening derangement before targeting definitive answers.

Download the Managing Emergency Cases in General Practice: UO, Hypoadrenocorticism, & Anaphylaxis Quick Reference (Free)
Want a concise, clinic-friendly summary you can save or share with your team?
Download the Managing Emergency Cases in General Practice: UO, Hypoadrenocorticism, & Anaphylaxis Top Takeaways PDF in an easy, printable format.
Missed the live CE?
You can still take the free course on-demand and receive 1 hour of RACE-approved CE here and check out our entire live and on-demand CE library here.
Complex cases are also easier when they are not managed alone. DVM STAT criticalists are available 24/7 for immediate phone consults on unstable patients, and full case reviews are returned in written consult reports within two hours.
Need Help Co-Managing Critical ECC Cases?
Through DVM STAT’s Emergency & Critical Care teleconsultations, primary care teams gain access to board certified internal medicine specialists who provide: Immediate phone consults by calling the STAT line 24/7/365 or submit through the DVM STAT portal to save time on the phone - receive a phone call within 20 minutes to discuss your case.
Case specific diagnostic guidance
Step by step treatment plans
Support for interpreting complex or conflicting test results
Follow up support to adjust treatment plans over time with the same criticalist for case continuity
Consults are available on demand and designed to support the veterinarian client patient relationship while improving patient outcomes.
Already have an account? Submit an Emergency & Critical Care teleconsultor Call the STAT line directly