
When Minutes Matter: A Criticalist's Approach to Canine Heat Stroke
In DVM STAT’s recent CE webinar on Heatstroke, Christina Whitley, DVM, DACVECC shared practical, evidence-based guidance on recognizing, stabilizing, and optimizing outcome in heatstroke in dogs.
Missed the live CE? You can still take the free course on-demand and receive 1 hour of RACE-approved CE here and check out our entire on-demand CE library here.
Summer in the ER has a rhythm. Lacerations, GDVs, foreign bodies, and somewhere in the middle of every heat wave, the collapsed Bulldog who was "just out for a quick walk."

Heat stroke is one of those diagnoses where the clock starts before the patient hits your door, and where the decisions you make in the first 90 minutes carry more weight than almost anything else you'll do for that animal. Mortality still sits between 50 and 56 percent in the published literature, and the patients who survive often need prolonged hospitalization with multi-system support.
This is a condition that rewards preparation. Here's how Dr. Whitley, board-certified criticalist and DVM STAT specialist, approaches these patients, distilled from her recent CE Hub webinar on heat stroke management.
What Heat Stroke Actually Is
Heat stroke is a life-threatening condition characterized by a temperature greater than 104°F that can lead to systemic inflammatory response syndrome (SIRS) and subsequent multiple organ dysfunction syndrome (MODS). It is not the same thing as a fever. Fever involves a hypothalamic reset. Heat stroke is a failure of thermoregulation.
Human medicine distinguishes a few related entities worth keeping in mind:
Heat stress: discomfort and physiologic strain, normal temperature
Heat cramp: sodium and chloride loss, normal temperature
Heat exhaustion: fatigue and GI signs, normal to mildly elevated temperature
Heat stroke: the life-threatening end of the spectrum
In dogs, we typically see two variations. Exertional heat stroke follows strenuous exercise, seizures, eclampsia, toxicities, tremors, or drug reactions like malignant hyperthermia. Working and sporting dogs are classic patients. Non-exertional heat stroke happens when ambient temperatures exceed the dog's ability to dissipate heat, often complicated by upper airway obstruction.
Why Dogs Are So Vulnerable

Dogs rely on four mechanisms of heat dissipation: radiation, convection, evaporation, and conduction.
Radiation and convection do the heavy lifting, roughly 70 percent of heat loss, until ambient temperature equals body temperature.
Once that threshold is crossed, those mechanisms fail and the dog is left depending on evaporation through panting and paw pad sweating, which accounts for the remaining 30 percent and which becomes increasingly ineffective at extreme temperatures.
Risk factors that compound the problem:
Obesity
Heavy fur coats
Lack of acclimatization
Brachycephalic conformation
Laryngeal disease
Geriatric patients
Sudden changes in exercise intensity
The "weekend warrior" pattern matters. A dog whose exercise habits change significantly over a two-week period is at higher risk than one with consistent conditioning.
The Pathophysiology in Plain Terms
When heat dissipation fails, cardiac output increases, peripheral vasodilation kicks in, and the dog becomes tachycardic in an attempt to shed heat. Direct thermal injury damages endothelial cells, triggering coagulation disturbances. Cytokines flood the system. Organ dysfunction follows.
The CNS takes an early hit through a combination of poor cerebral perfusion, direct thermal damage, cerebral edema, hemorrhage, and metabolic derangements like hypoglycemia. Coagulation pathways unravel acutely. The myocardium sustains direct injury. The kidneys face a triple threat of direct thermal damage, myoglobinuric tubular injury, and hypoperfusion. The GI tract, the shock organ in dogs, loses perfusion and barrier function, opening the door to bacterial translocation.
What You'll See on Presentation
The classic heat stroke patient arrives with abnormal mentation, possibly seizing, with petechiae or melena, injected mucous membranes, bounding pulses, and tachypnea. Temperature is often elevated, but not always, especially if the owners or referring clinic have already initiated cooling.
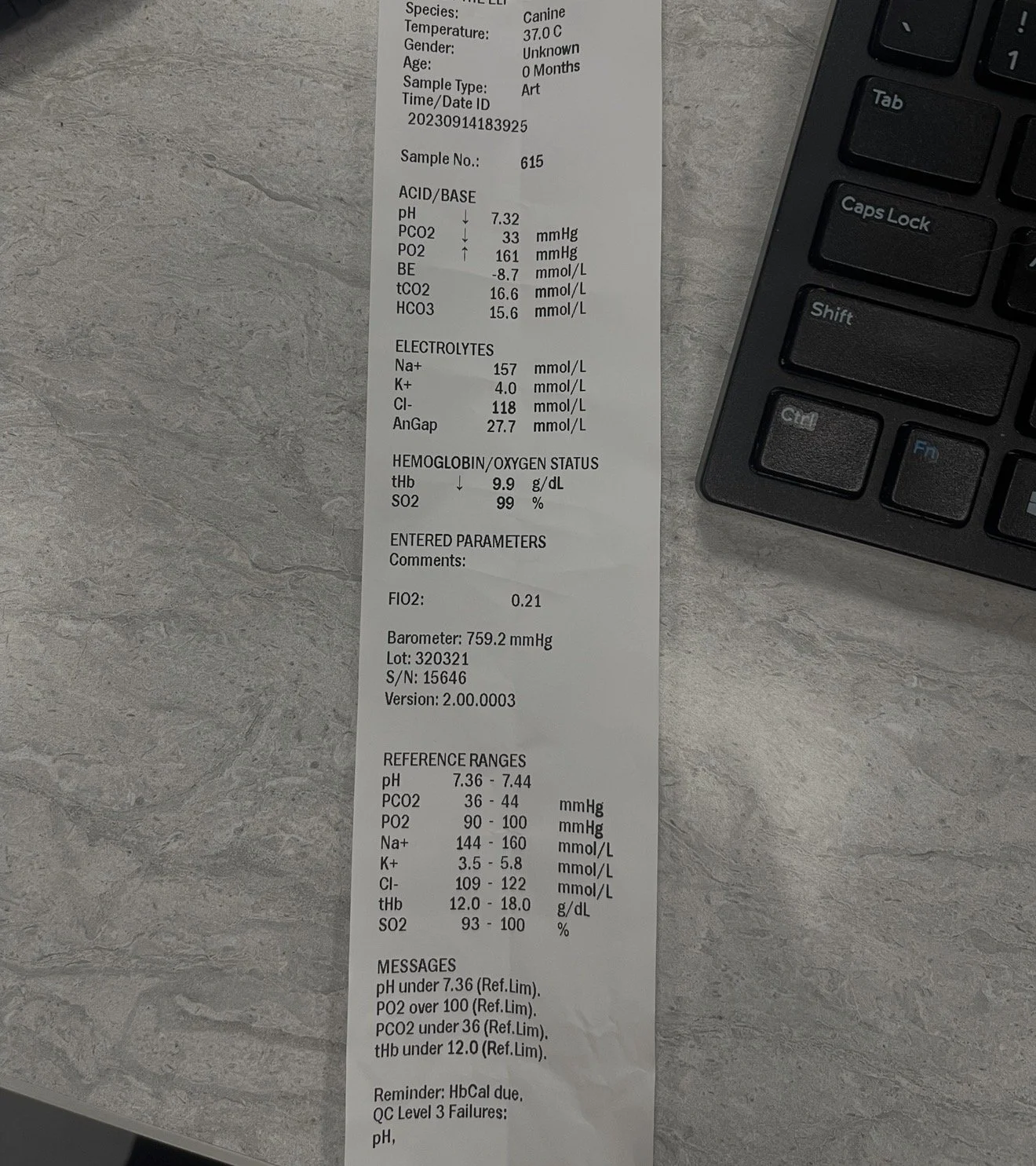
Minimum database first: PCV/TS, blood glucose, lactate. One important pitfall: hemoconcentration can falsely lower the glucometer reading. Don't assume normoglycemia from a borderline number in a clinically symptomatic patient.
From there, the diagnostic workup includes:
CBC (look for hemoconcentration, thrombocytopenia, leukocytosis)
Chemistry (azotemia, elevated liver enzymes, elevated CK, hypophosphatemia, hypokalemia, hypoglycemia)
PT/PTT
Blood gas if available (often respiratory alkalosis)
Urinalysis
Blood pressure, ECG
Serial monitoring is non-negotiable in the sickest patients. Q2 to Q4 hour rechecks of bloodwork and trends over 24 hours will tell you far more than any single snapshot.
Stabilization: What to Do, What Not to Do
Cooling. Tepid or cool water with fans, not ice baths. Ice baths cause peripheral vasoconstriction that paradoxically traps core heat. Stop cooling at 103°F to prevent rebound hypothermia.
Airway and breathing. Flow-by oxygen for most patients. If you hear stridor or suspect upper airway obstruction (brachycephalics, laryngeal paralysis), intubate early and cool aggressively. Watch for secondary non-cardiogenic pulmonary edema, pulmonary hemorrhage, and aspiration pneumonia. Get a chest radiograph.
Circulation. IV fluid support to restore perfusion and support renal function.
Neurologic support. Restore cerebral perfusion, monitor blood pressure, dextrose as needed, antiepileptics as needed (levetiracetam 30 mg/kg IV q8 is a reasonable choice). If you see prolonged seizures, anisocoria, or Cushing's reflex, consider cerebral edema and reach for mannitol if hemodynamically stable, or hypertonic saline if the patient is better hydrated. Avoid mannitol if there is concern for cerebral hemorrhage.
Coagulation. Consider fresh frozen (or liquid) plasma early, even with normal PT/PTT, if petechiae are present. Monitor coags every two to four hours.
Cardiovascular. Continuous ECG monitoring. Ventricular arrhythmias are common and often delayed, frequently appearing six to eight hours after presentation.
GI. PPIs, antiemetics, and broad-spectrum antibiotics to mitigate bacterial translocation risk.
Renal. Urinary catheter placement, urine output monitoring, fluid diuresis. Acute kidney injury can develop up to 48 hours after presentation. Dialysis may be needed in severe cases.
What the Numbers Tell You About Prognosis
Several findings carry meaningful prognostic weight. Negative prognostic indicators include:
Greater than 18 nucleated RBCs per 100 WBCs (a marker of direct thermal injury to bone marrow)
Ventricular arrhythmias
Seizure activity
Altered mental status
Obesity
Significantly prolonged PT/PTT (greater than 25 percent above normal)
Delayed therapy (greater than 90 minutes from onset)
Hypoglycemia
AKI with oliguria or anuria
The single best predictor of outcome is how the patient does in the first 24 hours. If they're trending in the right direction by hour 24, the prognosis improves significantly. If they're decompensating despite appropriate therapy, families need that conversation early.
The Real Takeaway
Heat stroke is a coordinated assault on every organ system. Treating it well means treating all of them at once, with the urgency the diagnosis demands and the patience that prolonged hospitalization requires.
For the general practice or ER team facing one of these cases without immediate specialty backup, this is exactly the scenario DVM STAT was built for. Real-time teleconsultation with a board-certified criticalist can help you sequence interventions, interpret evolving bloodwork, and have informed conversations with families about prognosis.
Want to go deeper? Dr. Whitley's full RACE-approved webinar, The Heat is On: Heat Stroke Management in Canines, is on demand through the DVM STAT CE Hub or directly here.
Download the Heatstroke Quick Reference (Free)
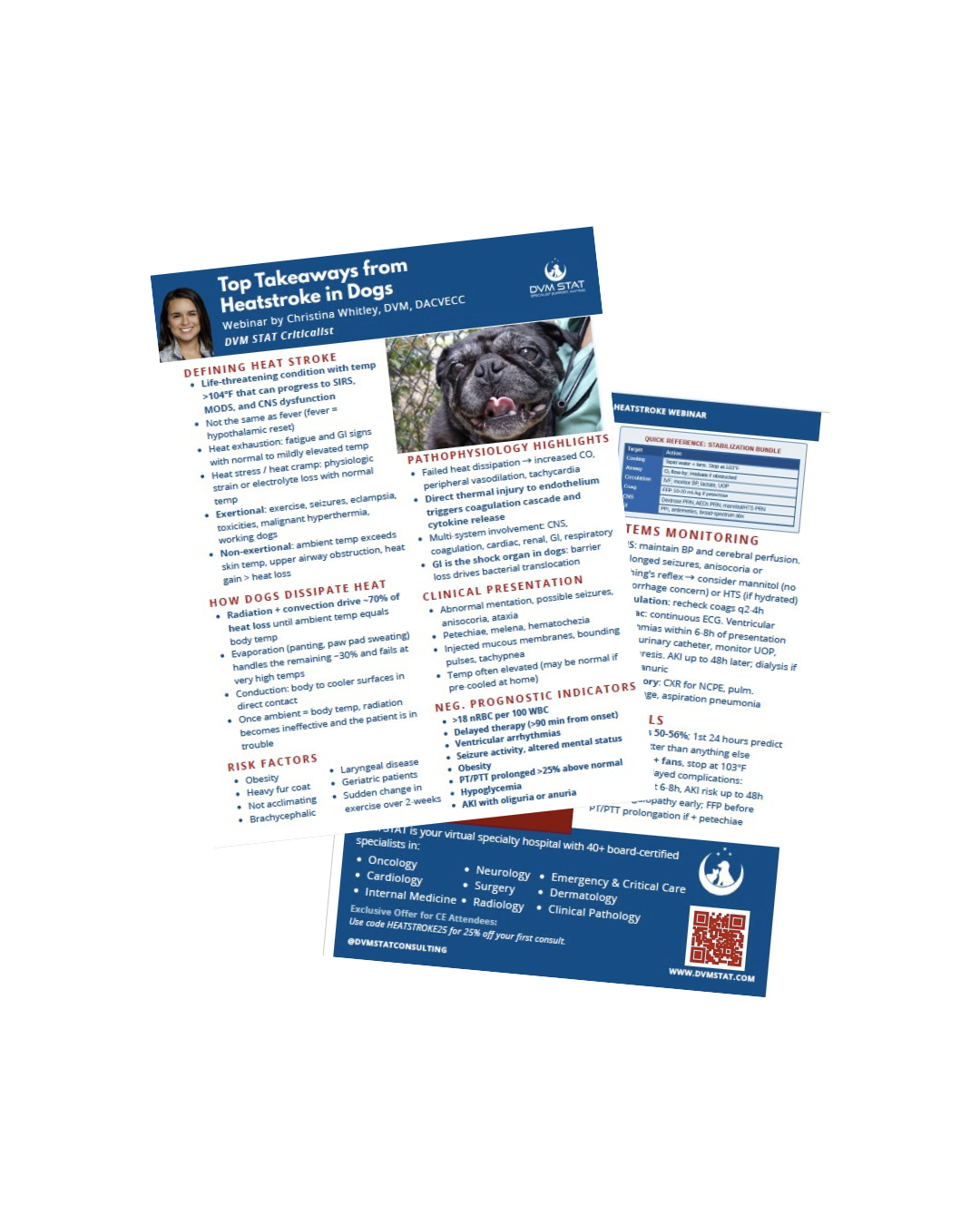
Want a concise, clinic-friendly summary you can save or share with your team?
Download the Heatstroke Top Takeaways Quick Reference PDF, which includes the key diagnostics, treatment recommendations, prognostic indicators and monitoring recommendations in an easy, printable format.
Need Help Co-Managing Critical ECC Cases?
Through DVM STAT’s Emergency & Critical Care teleconsultations, primary care teams gain access to board certified internal medicine specialists who provide:
Immediate phone consults by calling the STAT line 24/7/365
Or submit through the DVM STAT portal to save time on the phone - receive a phone call within 20 minutes to discuss your case.
Case specific diagnostic guidance
Step by step treatment plans
Support for interpreting complex or conflicting test results
Follow up support to adjust treatment plans over time with the same criticalist for case continuity
Consults are available on demand and designed to support the veterinarian client patient relationship while improving patient outcomes.
Already have an account? Submit an Emergency & Critical Care teleconsultor Call the STAT line directly!